The Problem Is Not The Grid
Hospitalist scheduling looks simple from far away. It is not. The hard part is not filling the shifts. The hard part is deciding who gets the unpleasant shifts, who covers which service, and how much disruption the group is willing to tolerate in the name of fairness.
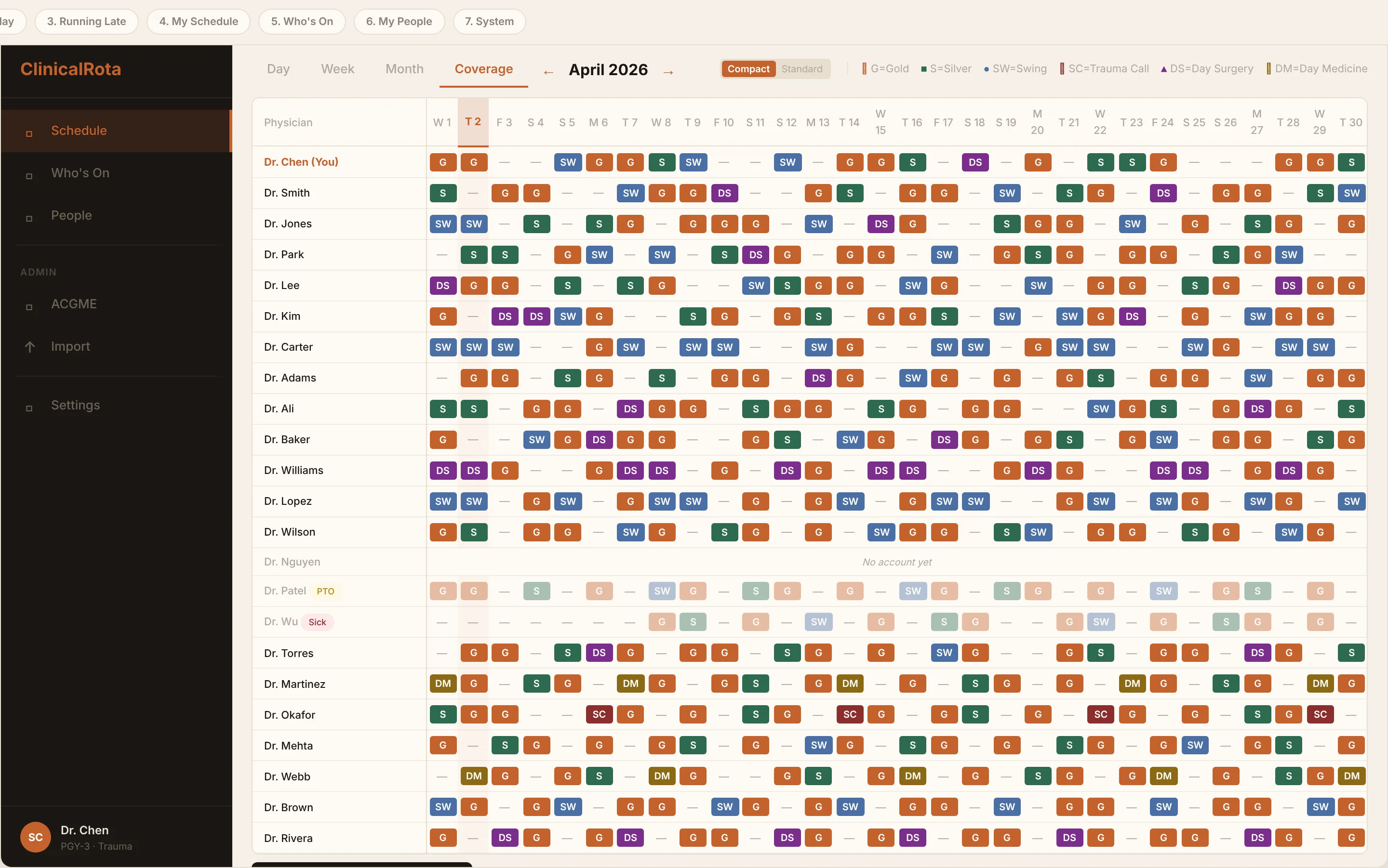
A lot of schedule tension comes from the fact that nobody can see the whole picture. Each physician sees their own nights, their own weekends, their own bad month. The scheduler sees the tradeoffs. The product question is how to make more of that logic visible without turning the schedule into a spreadsheet with better colors.