The ED Has Almost No Margin For Error
Emergency department scheduling is a different class of problem. A weak inpatient schedule can limp for a while. A weak ED schedule announces itself immediately.
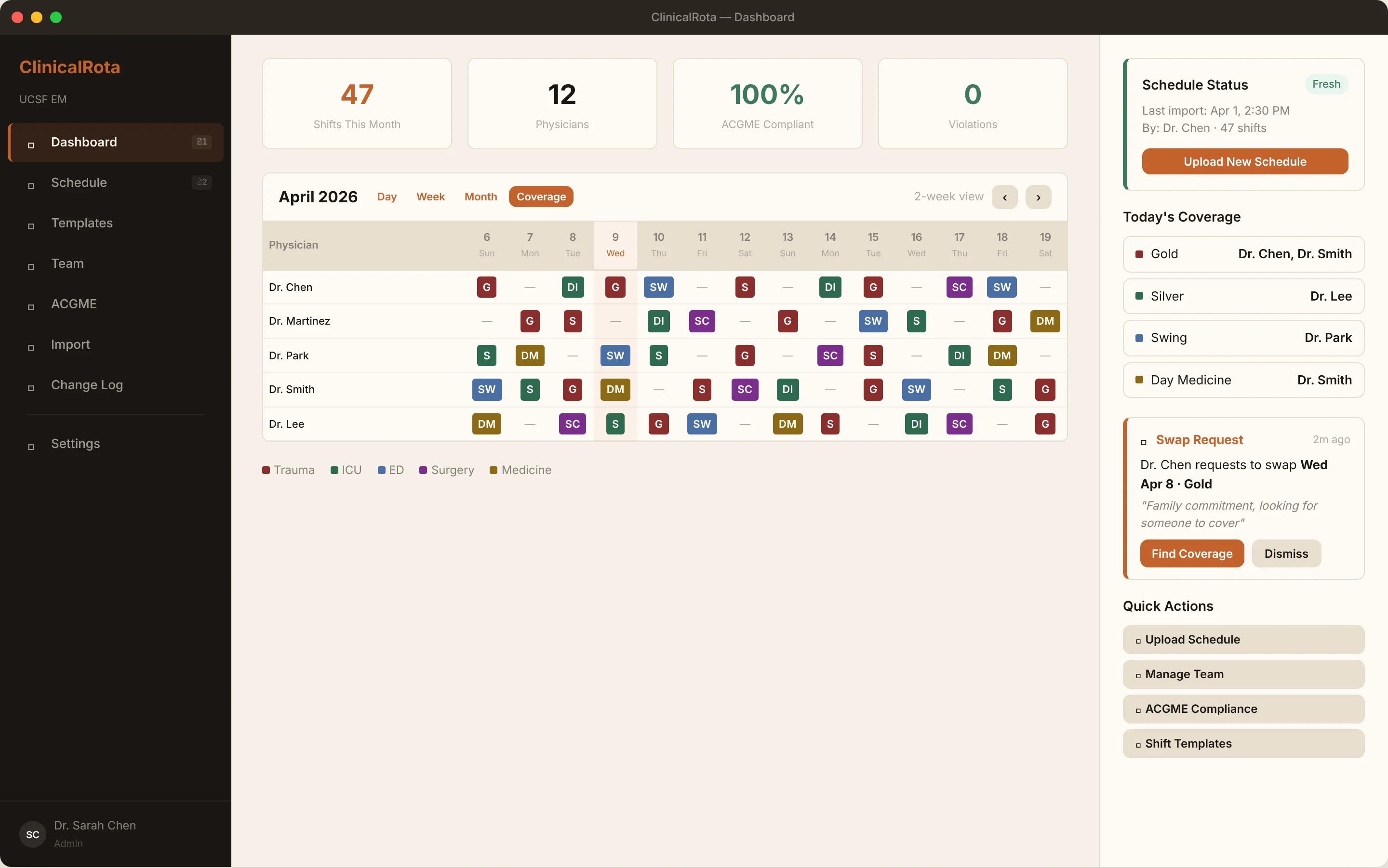
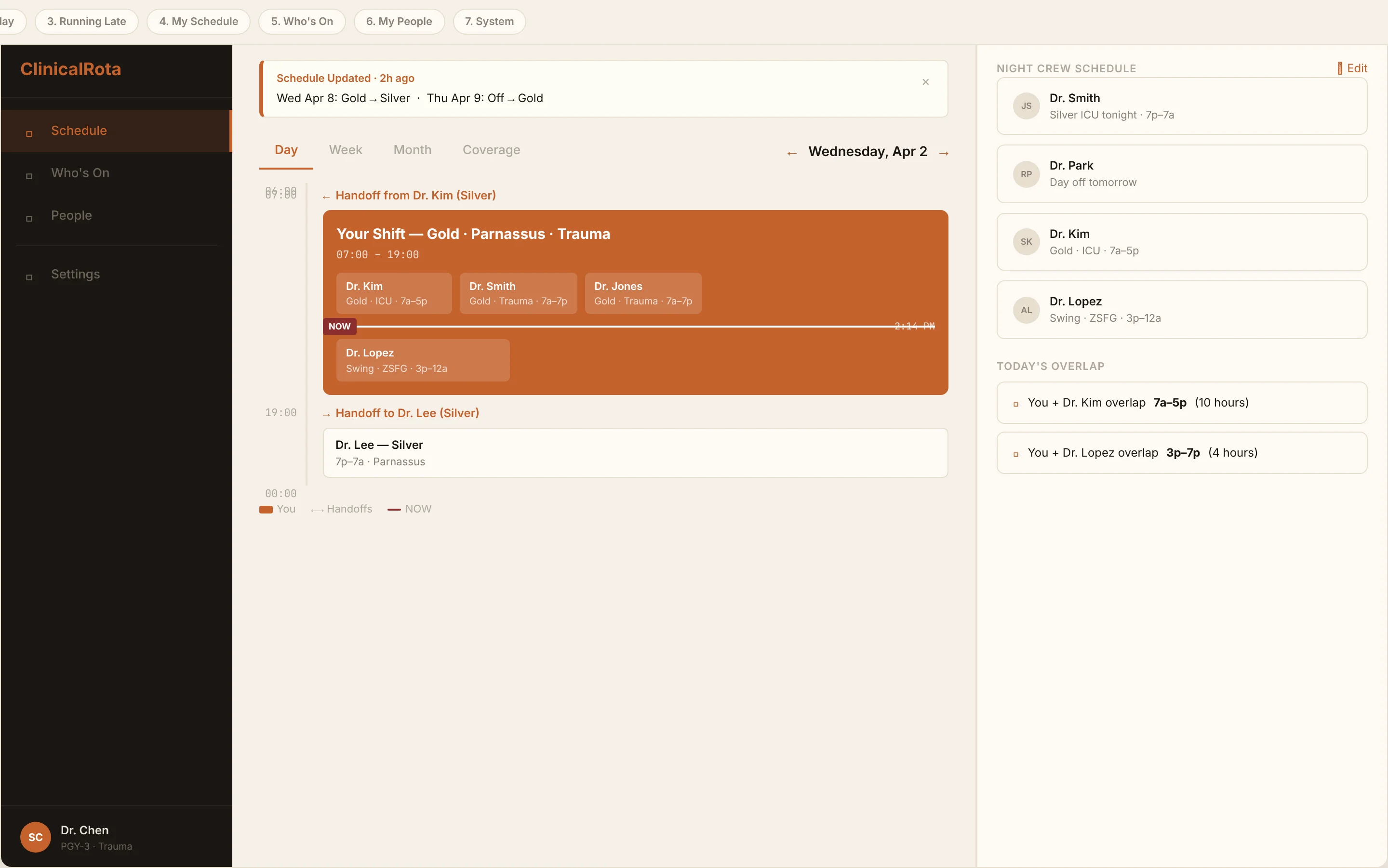
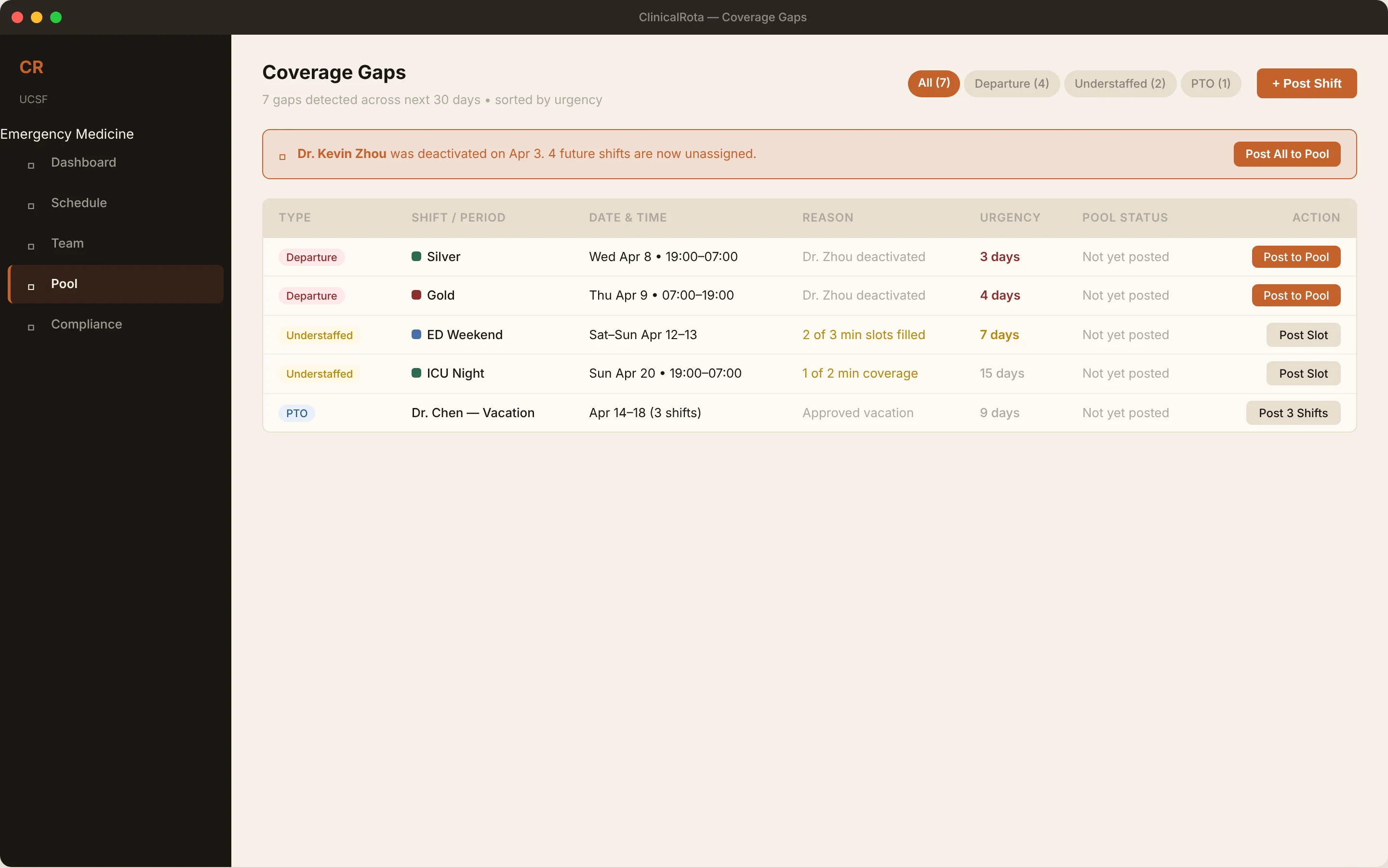
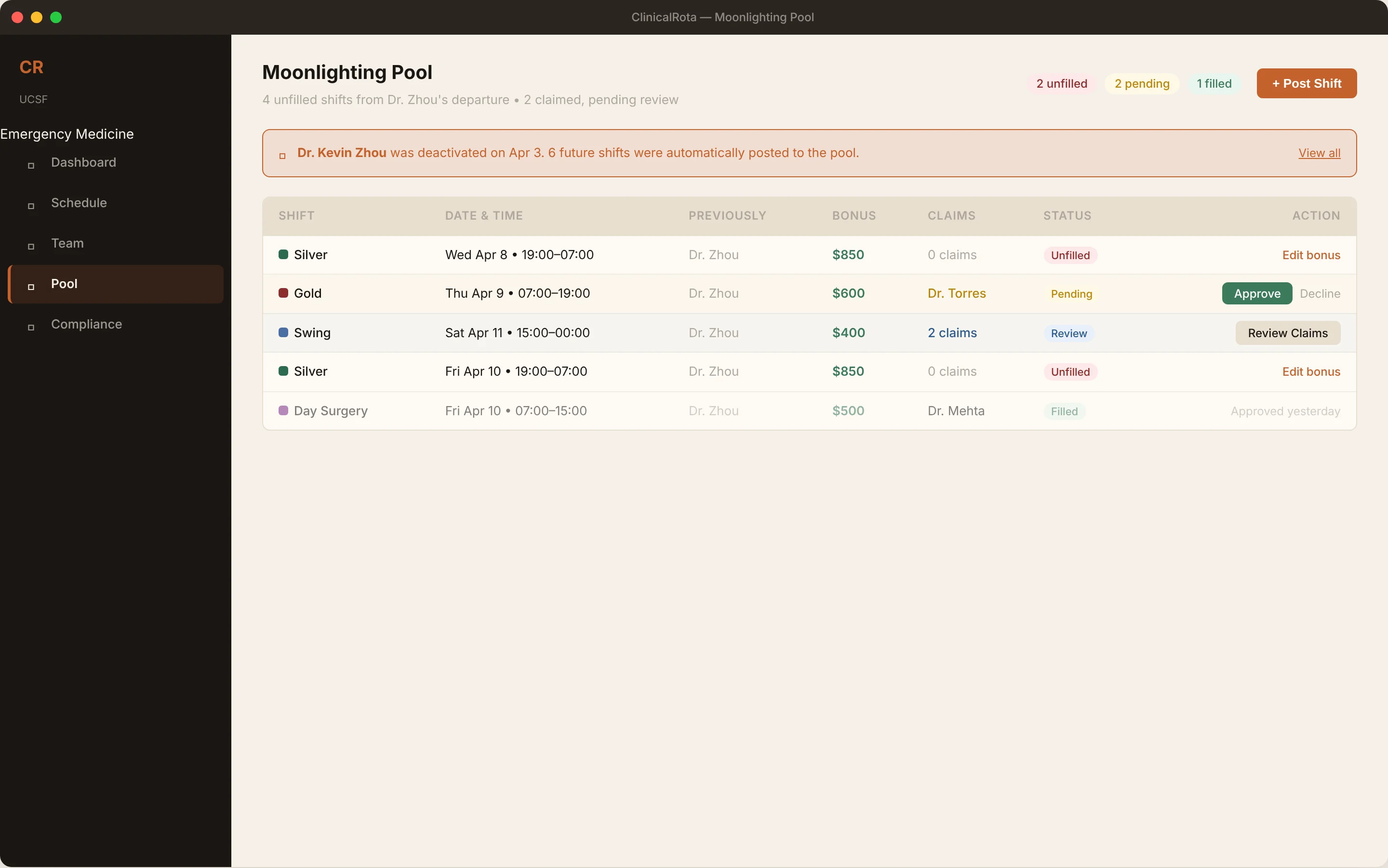
That changes what matters in the product. It is not enough to publish a monthly calendar. The useful thing is the layer underneath it: who is on now, who can replace them, where the handoff points are, and which parts of the week are one call-out away from trouble.